Vignette says a 60 year old male presents to the emergency department with complaints of fatigue, dizziness, lightheadedness and occasional near syncopal episodes over the past few days; He also complains of intermittent chest pain and shortness of breath on exertion since the past few days; He has a history of hypertension and takes losartan daily; On examination JVP shows cannon a waves; Vital signs show pulse rate of 35 beats/min which is slow and regular in nature, blood pressure of 110/70 mm of Hg, respiratory rate of 16 breaths/min, oxygen saturation of 96% in RA and temperature of 97.2 F; ECG shows wide QRS complex with no relation between P waves and QRS complexes however R-R intervals and P-P intervals are constant; Diagnosis?
Diagnosis is Third degree heart block.
Third degree heart block is characterized by a complete loss of communication between atria and ventricles (i.e. no impulse from atria passes through the AV node to the ventricles); JVP shows cannon A waves; ECG shows a wide QRS complex (ventricular escape rhythm) or narrow QRS complex (junctional escape rhythm) with no relation between P waves and QRS complexes however R-R intervals & P-P intervals are constant.
Causes:-
1. Idiopathic fibrosis or degeneration of the conducting system (i.e. Lev's disease)
2. Autoimmune disorders (e.g. SLE, systemic sclerosis)
3. Inflammatory conditions (e.g. myocarditis, Lyme disease, acute rheumatic fever)
4. Infiltrative myocardial disease (e.g. hemochromatosis, sarcoidosis, amyloidosis)
5. Electrolyte imbalance (e.g. hyperkalemia)
6. AV nodal blocking agents (e.g. beta-blockers, non-dihydropyridine calcium channel blockers, digitalis, adenosine, or amiodarone)
7. Anterior wall MI (due to extensive necrosis of the septum and conduction tissue i.e. His-Purkinje system)
8. Inferior wall MI (since right coronary artery supplies the AV node (i.e. right coronary dominant))
Presents with generalized fatigue, tiredness, lightheadedness, dizziness, chest pain, shortness of breath, near syncope and syncope. 3rd degree heart block is associated with polyuria (AV dissociation occurs as there is complete loss of communication between atria and ventricles in 3rd degree heart loss; this causes huge stretch in atrium leading to release of ANP which subsequently causes diuresis and polyuria).
Diagnosis:-
1. ECG shows a wide QRS complex (ventricular escape rhythm) or narrow QRS complex (junctional escape rhythm) with no relation between P waves and QRS complexes however R-R intervals & P-P intervals are constant.
2. Electrophysiology study.
Treatment:-
1. Temporary pacemakers (i.e. transcutaneous or transvenous pacing to increase the ventricular rate).
2. Insertion of permanent pacemaker (PPM).
3. Treat the underlying cause and stop the offending agents.
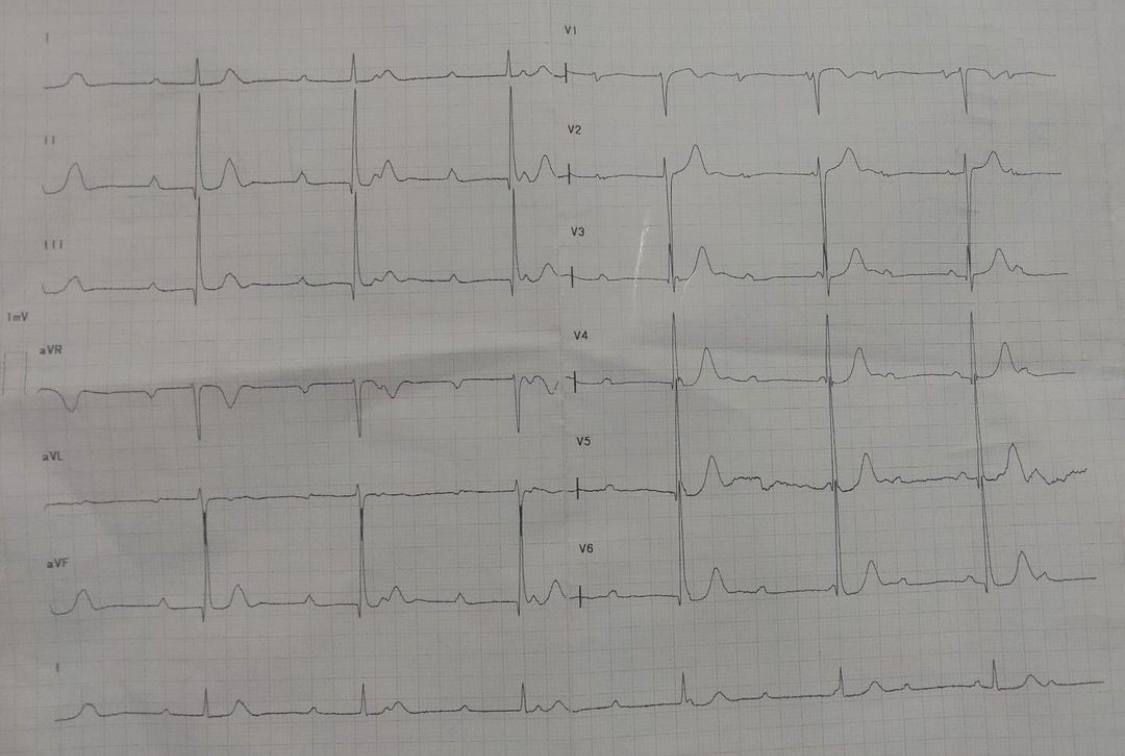
Figure:- ECG showing 3rd degree heart block